

I am not suggesting that CBCT should be used on every patient, but I am suggesting that with multiple rooted teeth, the sagittal & axial view provided by CBCT can save time and prevent endodontic complications, both of which provide justification for a more routine use of CBCT in endodontics. In our practice at SSE, the CBCT is not a profit center. We have priced these images to make them affordable to all patients. Our implementation of CBCT is to provide the highest quality of endodontic care available.
There has been some discussion about the indications for use of CBCT in endodontics. The AAE and AAOMR released a joint position statement regarding the use of CBCT in endodontics.
The section on patient selection criteria states, “CBCT must not be used routinely for endodontic diagnosis or for screening purposes in the absence of clinical signs and symptoms. The patient’s history and clinical examination must justify the use of CBCT by demonstrating that the benefits to the patient outweigh the potential risks. Clinicians should use CBCT only when the need for imaging cannot be answered adequately by lower dose conventional dental radiography or alternate imaging modalities.”
I would suggest that there are times when a clinician has no way of knowing what additional information a CBCT would provide prior to starting treatment. This information may often prevent complications, such as perforation, which potentially could affect long term prognosis.
This patient came to SSE for emergency treatment. #18 DX: Necrotic pulp w/ Symptomatic Apical Periodontitis. RCT initiated. 3 canals located, however a 4th distal canal is not found. 2 distal roots are apparent the pre-op film. The ML, MB and a distal canal are located. The distal is opened looking for the 4th canal. After 20-30 minutes of searching for 4th canal, the patient is re-appointed for 2 step treatment.
Upon return for second visit, the symptoms of SAP have not completely resolved. Slight vestibular swelling noted. We decided at that point to take a CBCT to help us located the 4th canal.
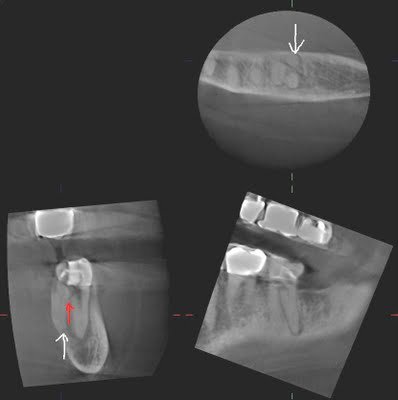
The CBCT clearly shows us that a perforation has been created (red arrow), and the additional canal/root is lingual to the DB canal. A sagittal view, provided only by CBCT, can provide information that is not available by conventional radiography.
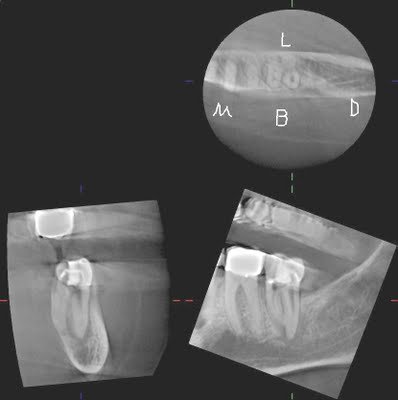
With these images, the 4th canal is easily located within minutes of opening the tooth.

In this case, a CBCT provided valuable information that identified location of the 4th canal. If taken prior to starting, the 4th canal would have been located more quickly and without the small perforation in the distal.