
Rather than try to have an overarching theme to this post, I will present each of today’s patients as each case was complex and each illustrate rather important points. For the sake of brevity, I will only post significant findings (and I apologize for poor consistency and errors in grammatical tense) . Unless otherwise stated, assume medical history is non-contributory. I would love for readers to post feedback, alternate treatment plan ideas, or other approaches to these cases.
Patient 1:
This patient presented with a history of root canal treatment on #20 by an endodontist 1-2 years ago. #19 was treated by her general dentist ~8 months ago, and #18 was fractured and replaced with an implant within the last two years. The crown came loose and was replaced with a post 1 month ago. Following this treatment, she described severe pain upon chewing and swelling on her tongue side of the tooth. There is no extraoral sign of swelling or lymphadenapathy. No intraoral swelling or sinus tract. Around #19, the gingiva is edematous and inflamed with bleeding on probing. The crown margins are open and overextended. The probing depths on #19 are 3 mm interproximally and 8-9mm mid buccal and mid lingual. The radiograph reveals a laterally widened PDL with a hint of an apical radiolucency. The restoration on the mesial is into the furcation and associated with horizontal bone loss. #20 displays an apical radiolucency as well. The implant on #18 is bulbous and overcontoured to the mesial with some signs of horizontal bone loss.

Unfortunately, I recommended extraction of #19 due to the likelihood of a vertical root fracture and a poor restorative prognosis. I recommended she return to her previous endodontist for reevaluation/recall of #20. I also provided her some proxibrushes to maintain oral hygiene around #18. Would you rather have that root canal/crown or that implant…or neither?
Patient 2:
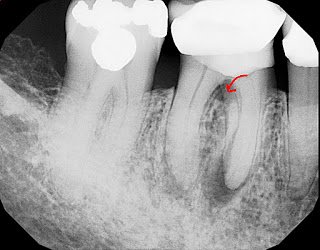
This patient is referred by her general dentist for evaluation of #3 and initially presented two weeks ago. She reports having root canal therapy a year and a half ago by another local endodontist, no microscope. Since the time of treatment, she has had spontaneous “shooting” pain that is localized to tooth #3. It is worse in the morning and with mastication. A history of symptoms indicates that the tooth was likely vital preoperatively and so persistent bacteria is not a feasible etiology. No extraoral swelling or lymphadenopathy. No intraoral swelling or sinus tract. Probing depths 2-3mm, crown margins are in tact. Occlusion is light in MI with no interferences. No palpation tenderness, no swelling, no sinus tract, no percussion tenderness, no mobility. Slight bite pressure tenderness on the MB cusp and P cusp only.
Preop, no radiolucency, slight ligament widening in the palatal, short palatal obturation, overenlarged mesial obturation in the cervical third, undermined/weakened mesial tooth structure. Diagnosis: previous treatment/acute apical periodontitis. Possible etiology: restorative recontamination, root fracture, strip perforation of MB/MB2. I recommended retreatment but cautioned that a finding of a root fracture would indicate a need for extraction.
Upon access, blood was found on the palatal canal, and, in spite of anesthesia, the GP was tender to pressure with fluid built up around it. No fractures were found. Additionally, a strip perforation was found in the cervical third of MB2. It was repaired with MTA and the palatal canal was retreated. The patients symptoms resolved immediately, and the case was finished this morning.
This patient went to her new dentist for a broken restoration on #30. Decay was found encroaching on the pulp chamber and she was referred for root canal therapy. She is asymptomatic. #31 was treated 2 years ago by another endodontist, no microscope. The anatomy appears to be very challenging. A history of symptoms of cold sensitivity and throbbing pain prior to the previous treatment indicate that #31 was likely diagnosed as irreversible pulpitis preoperatively.
Treatment on #30 was completed at today’s visit and treatment options for #31 were discussed. Restoratively, the case is compromised with a crown on a buildup with voids. Additionally, retreatment of the mesial root is going to be challenging if not impossible. If, as it appears, the distal root is the primary source, retreatment may be successful. One alternative, if retreatment is not successful, is to place spacers to loosen the tooth and then try an intentional reimplantation. Apical surgery is difficult to impossible in this location with such long roots (25mm working length on #30).
Asymptomatic, original treatment over 15 years ago. Her crown and posts came off and extensive recurrent caries was found beneath. Her dentist cleaned the area and placed a temporary crown before referring her for evaluation. While radiographically, the ligament is in tact, her history indicates bacterial contamination and retreatment was recommended.
This patient is asymptomatic. She recently moved here and her new dentist noted a parulis buccal to #30. She is ~85 years old. Probing depths were 2-3mm with bleeding on probing and a class 1 furcation involvement. The margins on the composite were open. Due to the compromised restorative prognosis and the furcation radiolucency, I recommended extraction. She does not wish to replace this tooth at this time, but an FPD is likely her best option. She is fortunate to have full molar occlusion on her left side.
I hope that our readers learned something from these cases. You will probably realize that I started no new root canal treatment today, and that all our cases were complex diagnostically and involved molars. This is typical for our practice.
If you have any input or questions, please voice them in the comments, but please remain constructive. As always, I invite readers to see more cases posted regularly on our facebook page at www.facebook.com/alpharettaendo.
If you have any suggestions or requests for future posts, please leave them in the comments!