

Occasionally, as an endodontist, we are referred a patient for a difficult, maybe questionable, save. This patient was 85 years old and was undergoing cancer treatment. He was referred late one afternoon for treatment of #32. The referring dentist had started the root canal treatment earlier in the day and had stopped due to difficulty locating the mesial canals. The patient arrived with his tooth anesthetized and with IRM in the access. Tooth #32 is the distal abutment of a longspan FPD, and the dentist was confident that it could either be saved or a new FPD fabricated and fit.
Upon access, it was immediately clear why the tooth was a challenge for the referring dentist (if being a tilted third molar bridge abutment on an elderly patient wasn’t enough). The mesial gingiva had overgrown beneath the FPD and there was still caries everywhere. Both saliva and blood were flooding beneath the rubber dam and into the access.
After cleaning the caries, resecting the gingiva, and controlling the hemmorhage with astringedent, I called the general dentist on his cell phone to have his restorative input. There was minimal supracrestal tooth structure remaining on the mesial, and I questioned the restorability of the tooth. The dentist was dismissive of any alternatives and confidently requested I complete the treatment.
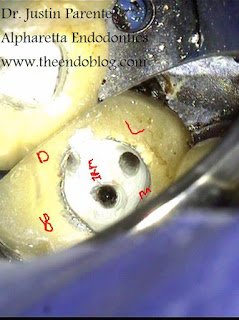
At this point, something needed to be done to maintain a clean dry field. It became clear very quickly that our normal ancillary use of Oraseal calk was not enough. I had my assistant maintain a steady stream of air on the tooth while I inserted size 6 hand files into the two mesial canals, and a size 30 file into the distal canal. I would recommend lubricating the files with vaseline before placing them. I then maintained the air stream while my assistant mixed up a loose batch of IRM. I placed the IRM and compacted it within the access and around the files before trimming back the material that flowed out beneath the crown.
As the IRM set, I moved the files in a circular patterns to prevent them from locking in and to create a funneled pattern of space. Upon setting, I removed the files and was left with perfect pathways. Through these, I did my cleaning, shaping, and obturation.
This technique can be applied to any situation in which caries is removed beneath a fixed restoration, and the restoration is to be maintained to hold a rubberdam and act as a temporary.
If you have any questions or clinical tips to share of your own, please post them in the comments below.
Also, if you are new to the blog, you can also see more of my cases on my office’s facebook page: www.facebook.com/alpharettaendo
Thank you!