
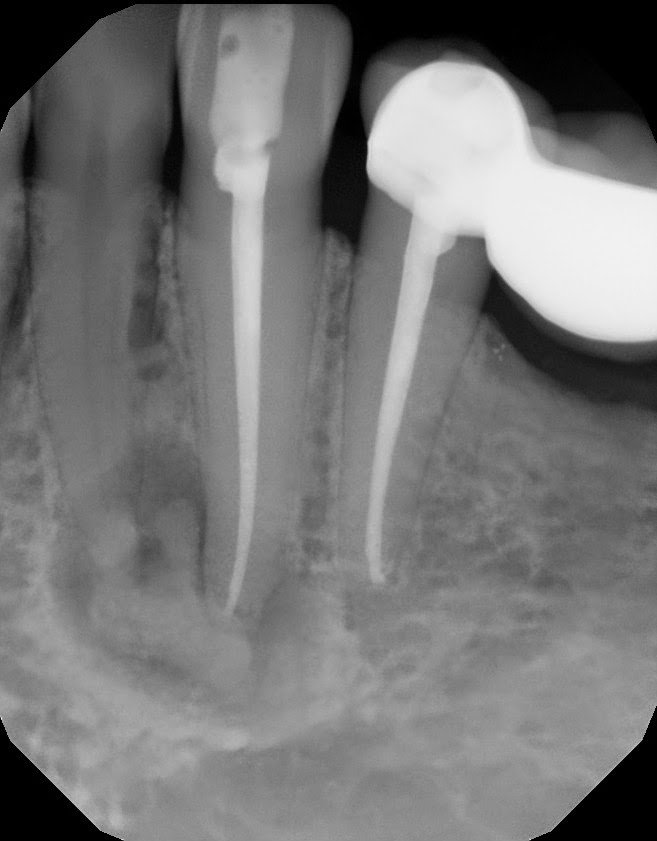
A 42 yr old, white, female presented for evaluation of #22. She was asymptomatic, with a prior RCT on #22. A large nodular, irregular, radiopacity found within a large radiolucent area on the periapical radiograph. Tooth is normal to palpation, percussion and probings.
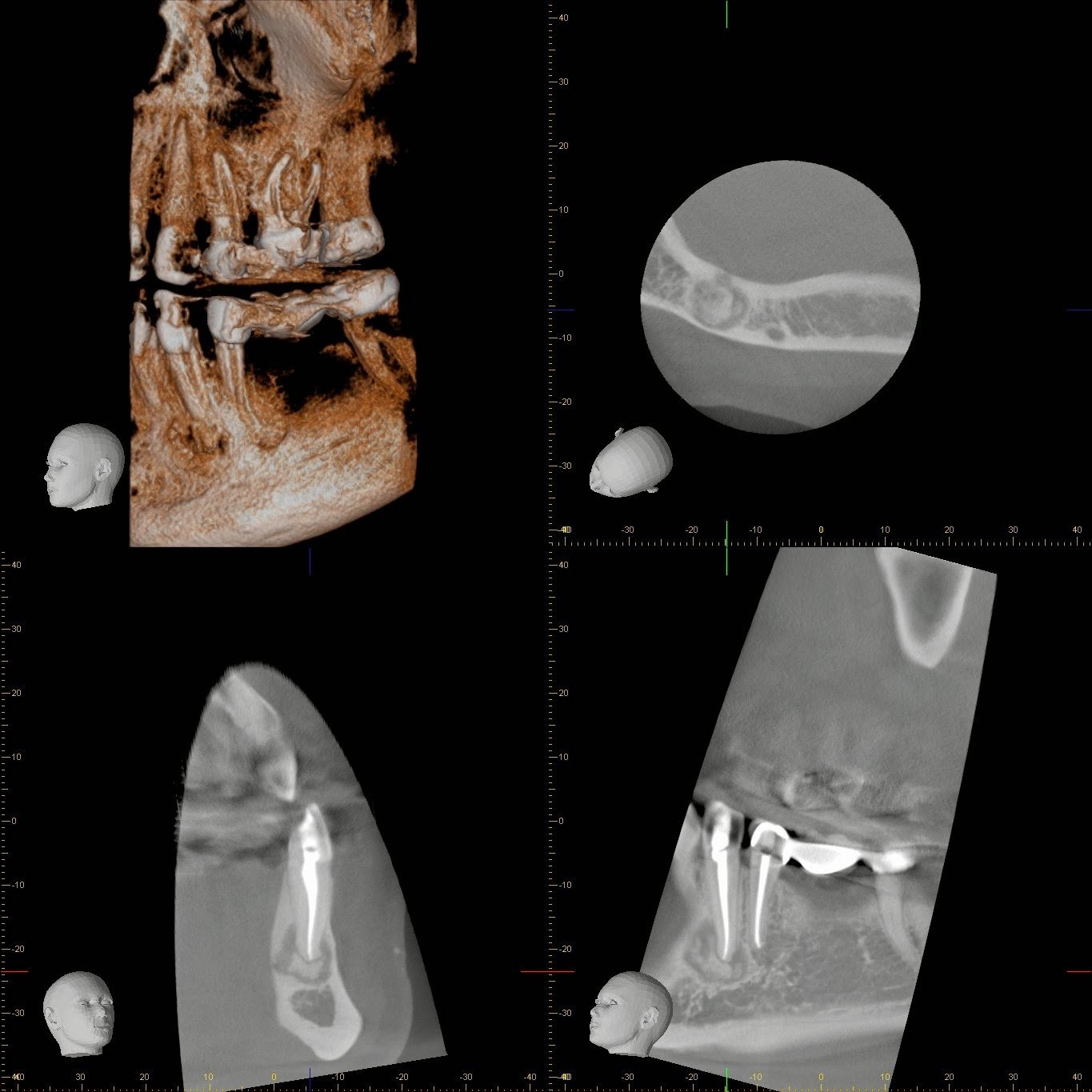
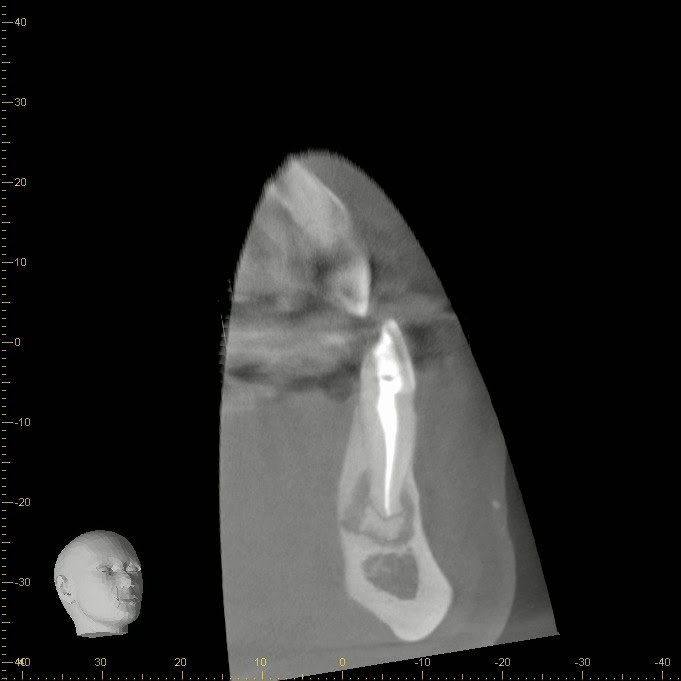
DX: Prior RCT with possible periapical cemental dysplasia. Apical surgery recommended with biopsy.
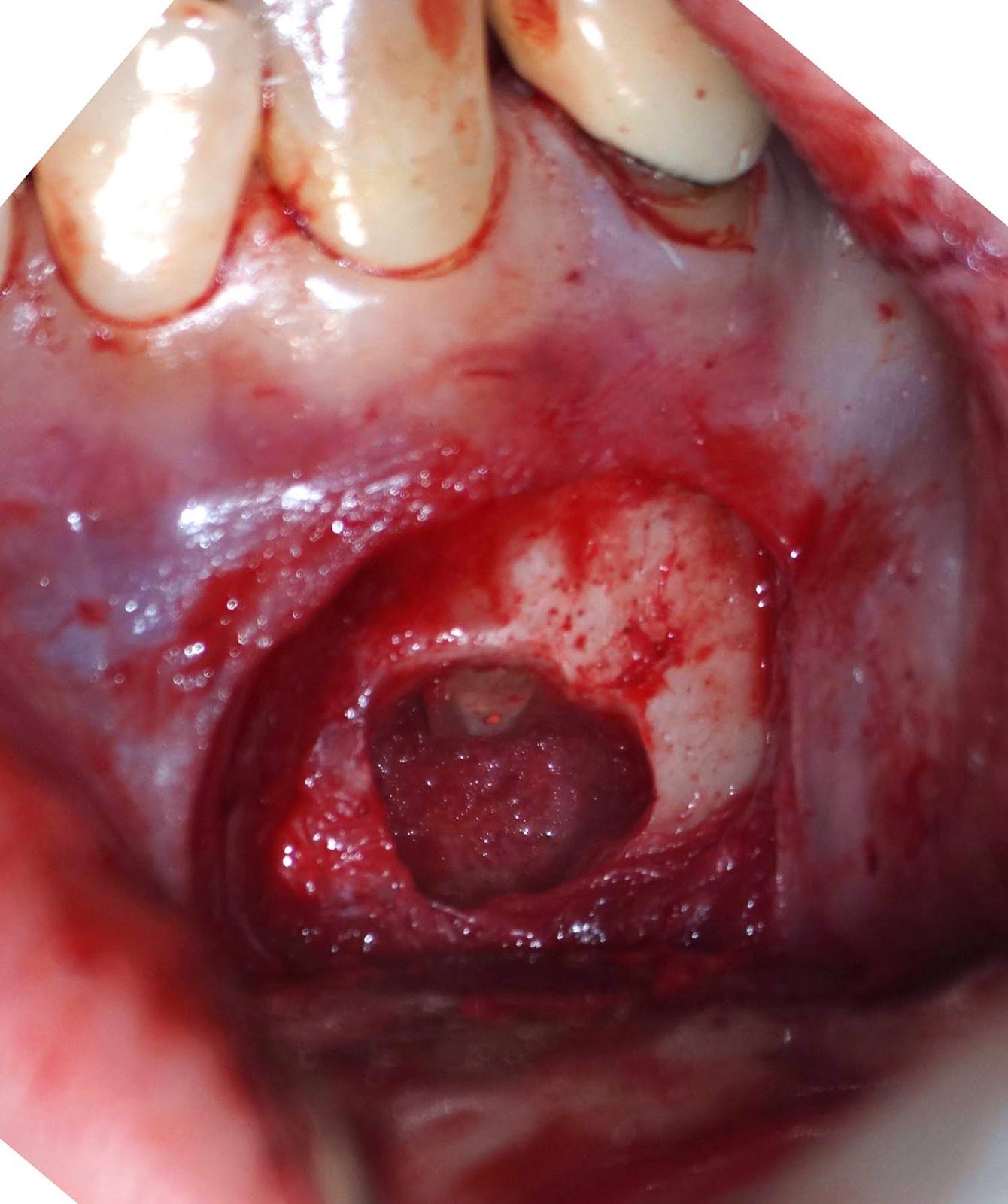
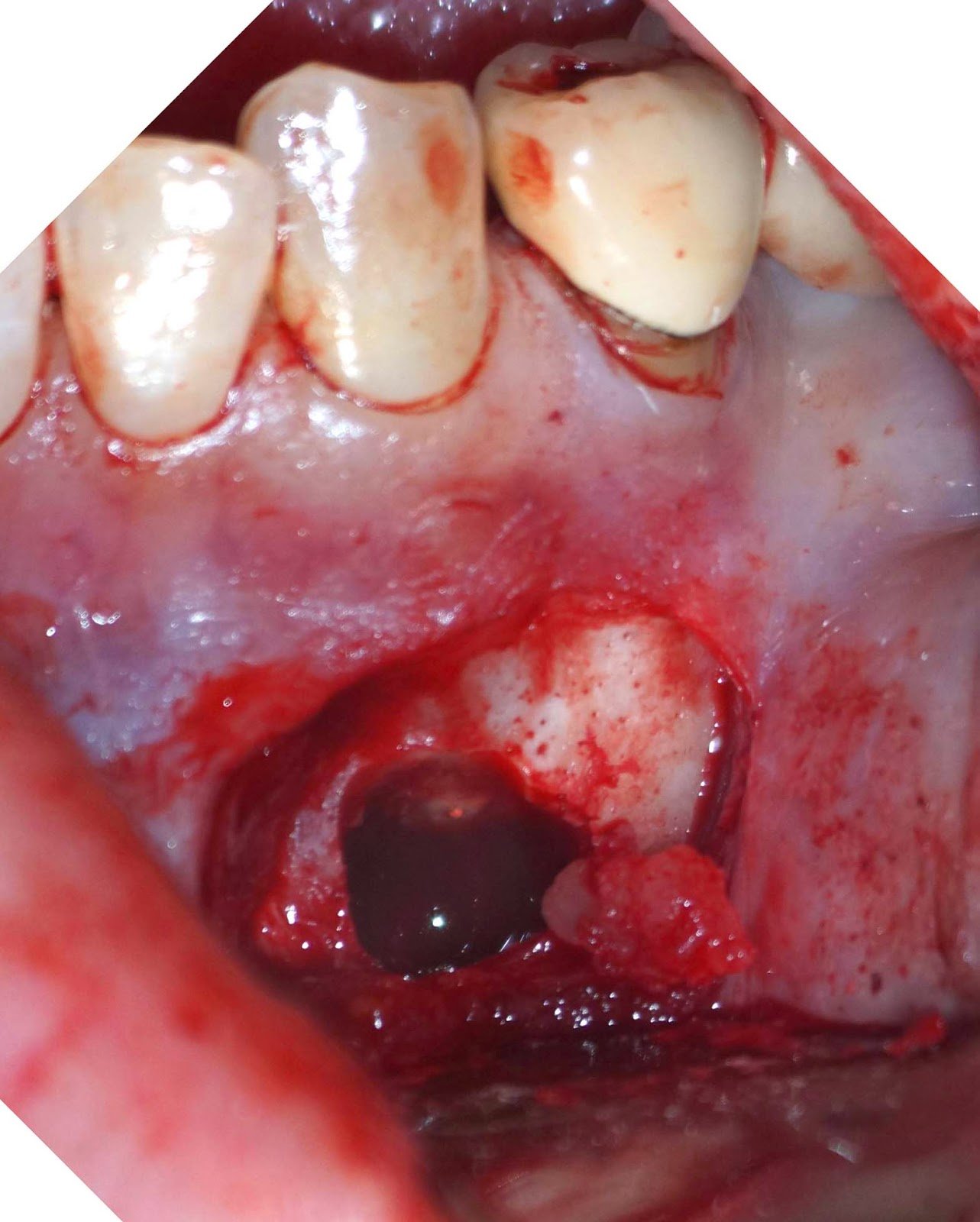


Biopsy report indicated Periapical Cemental Dysplasia (anterior focal osseous dysplasia) Recurrence would be unusual, but other areas of dysplasia can arise as well as truamatic bone cysts are also common.